
Pain That Won't Quit? A Neuro Lens on Tactile Mapping and Why “Touching It” Isn't the Same as Training It
If you work with persistent pain long enough, you meet THAT client.
They've tried everything. The program was solid. The soft tissue work happened. They stretched, strengthened, rested, 'fixed their posture.' And somehowwww the pain is STILL there.
So here's the question I ask myself when I hit that wall:
"What if the issue isn't only the tissue, but the brain's map of it?"
SAY WHAT?
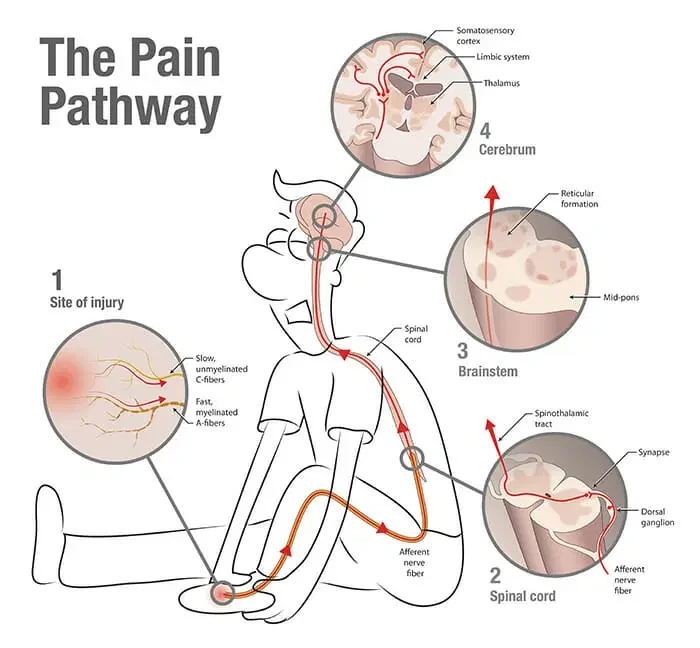
Sometimes just the MAP alone is the place to focus on. When pain persists, the nervous system often changes how it processes sensation from the painful area, and one of the most practical gateway drugs... (I mean TOOLS LOL) into that reality is tactile mapping. What I mean is how clearly someone can feel, localize, and discriminate touch. A systematic review in The Journal of Pain found evidence that tactile acuity can be diminished in several chronic pain conditions, including arthritis, complex regional pain syndrome, and chronic low back pain, which supports the idea that sensation can get 'fuzzier' in persistent pain presentations.
So if this is true, why not give it a go and try to un-diminish it? Ya picking up what I am putting down?? Blurry maps create blurry confused signals, which make the brain not very happy or safe enough to move with freedom. And that is exactly what our clients want, right?
PhysioPrescription "Chronic Pain: All in my head?"
The Short Version of the Neuro Idea, in Normal Human English
Your brain is constantly building a map of your body using incoming sensory input. When that map is clear, movement tends to feel more predictable, coordinated, and safe. When the map gets noisy or less precise, the body often compensates with protection, and that can look like guarding, bracing, tension, a flushed face, increased blinking, increased breath rate, and ongoing pain.
That 'blurry map' can show up like a client who says:
• They feel pain but cannot describe it well
• They feel disconnected from the area
• They hate being touched there
• They cannot tell exactly where they're being touched
• Their symptoms are wildly inconsistent depending on context, stress, and attention
If you ask them to point to where it hurts and they wave their hand over a whole region, that can mean anything from a visceral issue to a poor map, so in this case more questions are always better.
Why Rubbing the Area Can Feel Good, Yet Not Change the Pattern Long Term
Touch can absolutely help someone downshift, and I am not here to shame manual therapy, self-massage, or any of the things that help your client feel safer in their body. I would get bodywork weekly if I could, honestly.
The distinction that matters is whether you are simply providing sensation, or whether you are training the nervous system to perceive sensation more accurately and appropriately. The intention and goal is everything.
A great paper on chronic limb pain found that tactile discrimination was associated with reductions in pain, whereas tactile stimulation alone did not produce the same effect. This is a big deal for movement professionals because it suggests that the LEARNING component of sensation can matter, not just the sensation itself.
So yes, rubbing can feel soothing. And at the same time, if the brain is still not confident about what is happening in that region, the protective strategy may remain the same. But hey, we gotta start somewhere right? Each new action leads us to a different path, and this blog is simply here to contribute to your thought process.
What Sensory Discrimination Training Actually Means (Without Making It Weird)
Sensory discrimination training is an intentional practice that asks the client's nervous system to do a cleaner job answering questions like: where is the touch, which direction, how many points, what changed, and can you identify it?
It is 'simple,' yet surprisingly powerful. There is also research in clinical pain populations showing tactile discrimination training can improve tactile acuity and is linked with meaningful changes, including studies in phantom limb pain and CRPS contexts where training has been associated with improved two-point discrimination. Visual context during training can also influence the effect.
You don't need any fancy equipment. What you have lying around or your two fingers is a great place to start.
4 Steps to a Simple, Ethical, Movement-Pro Friendly Way to Explore Tactile Maps
Here is a way to do this that does not require fancy tools, does not require you to become 'the touch therapist,' and stays inside a professional scope. Of course this is a free blog on the internet, please be an adult and do things within your licensure. Do not skip any of these steps even if they seem simple, stupid, or irrelevant.
Step 1: Set the Frame and Get Consent
You might say something like: 'Let's try a quick sensory check to see how clearly your brain is perceiving information in this area today, because clearer input oftentimes changes the way your body experiences pain and executes movement. If something feels too threatening, simply lift your hand or say stop. Let me show you on my own body first.' Then you demonstrate on your own arm or leg. They can watch you before they feel like it is okay to do that day.
That one sentence is doing a lot. It creates agency, reduces threat, and keeps you from accidentally turning it into a pass-fail moment. We want them to feel empowered, educated, and brought along the journey WITH you, not someone who just lies there while you 'fix' them. No thank you.
Step 2: Pick Your Baseline Metric
Pick one movement or outcome that matters to THEM and is easy to repeat: a squat depth, a hinge, a step-down, a reach test, cervical rotation, grip strength, or simply their pain on a scale of 1 to 10.
Picking a meaningful baseline before you do the drill is what separates a cool party trick from an actual clinical tool. You need to know what you are changing. Do not skip this step. I highly recommend documenting this to show them at the end of the session.
Step 3: Do a 60 to 120 Second Discrimination Drill
Choose one option and keep it calm.
Option A: Have them close their eyes, lightly touch one spot, and ask them to point to where they felt it. Watch whether they overshoot, hesitate, or consistently miss.
Option B: Left vs. right or up vs. down. Touch once and ask 'left or right,' or draw a tiny line and ask 'up or down.' The point is not to stump them, the point is to give the system a clean, simple discrimination task. Start on an area not related to their pain. If they are coming in for hip pain, start on their opposite arm to build trust first.
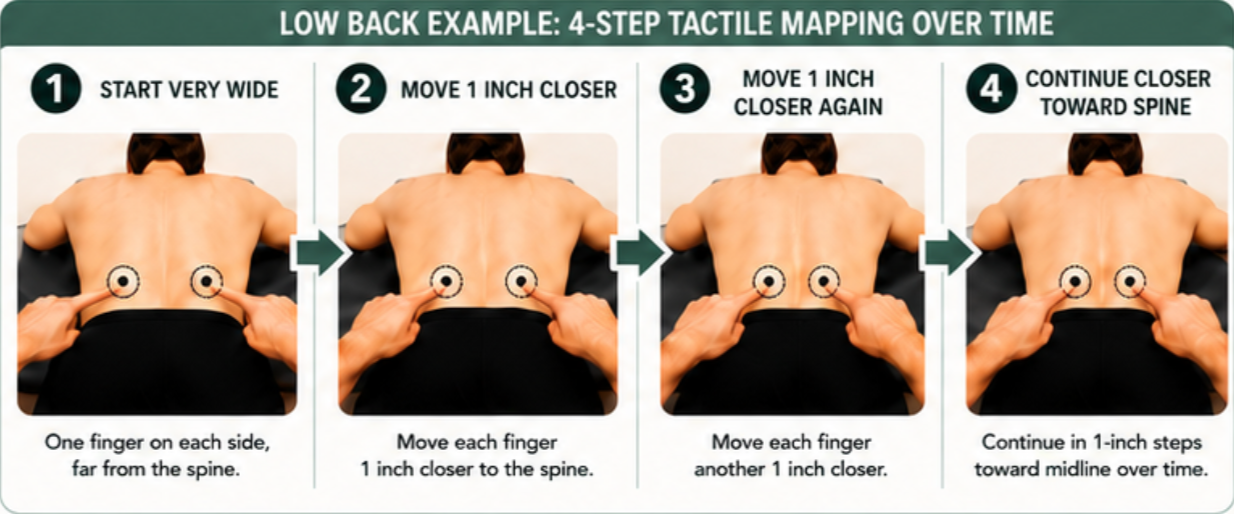
Option C: Two-point style work without fancy calipers. Use two fingertips close together OR one fingertip and ask 'how many fingers do you feel? One or two?' Then change the spacing slightly, usually lateral to medial or distal to proximal. Keep this gentle and appropriate to the client, especially if the area is sensitive. Refer to image above as an example.
If the person has high fear, or a history where touch is loaded with threat, scale way down, choose a less threatening region first, or skip it entirely. The goal is clarity and safety, not intensity.
A real story, because this still makes my jaw hurt:
After my sister's brain surgery, they would have her stand on a balance ball and throw a medicine ball at her to 'improve her balance.' I wanted to scream and cry and shake them. A person who just had brain surgery. You think THAT is a good idea? Bringing a cup of water to her mouth was hard enough for her, let alone an unstable surface with an object coming towards her. My jaw and neck hurt just writing this out to you.
The point: a harder exercise on a threatened nervous system often just drives a stronger protective strategy. MORE threat. Not less.
Step 4: Reassess Immediately
Retest the baseline movement or outcome right away. This is how you learn whether sensory clarity is a useful lever for that client on that day.
If nothing changes, no problem. You just learned something. If something changes, you now have a practical layer you can place strategically into warm-ups, resets, or between sets, especially for clients who get stuck in guarding patterns.
What to actually document:
• A photo or video of the baseline movement before and after
• A body diagram where you marked touch locations and accuracy
• A 1-line note: did the reassessment change? yes / no / neutral
That's it. Doesn't have to be fancy. It just has to be consistent. I also highly recommend drawing directly on clients (if they approve) so they can visually SEE the change. We can't always rely on them to tell us it FEELS different, you know?

Why This Can Help Movement Quality Without You Changing the Program
When sensory discrimination improves, even slightly, the nervous system often uses a different movement strategy because the input is less threatening. A less threatened system tends to spend less energy on protection. In plain terms, if the brain can locate and interpret what is happening more accurately, it often has less reason to protect and create the sensation of discomfort or pain.
That does NOT mean you abandon strength, mobility, or tissue capacity work. It means you have another lever to support them so that the training you are already doing lands better.
Common Mistakes I See Movement Pros Make With This
The most common pitfall is accidentally turning sensory work into a threat party, either by moving too fast, doing too much, or acting like the client is 'failing' when they cannot discriminate well.
The other pitfall is using random stimulation without a discrimination task and then wondering why it did not translate.
Keep it simple. Keep it short. Keep it consent-based. And always tie it back to a reassessment so you can see whether it matters. Keep tying it back to THEIR goal, not yours.
A Note Before You Go
The tissue matters. I am not here to throw out your whole program. But if you have been doing everything right and the pain is still hanging around, start asking what the map looks like.
Sometimes the most impactful thing you can do is not add a harder exercise. It is give the nervous system a cleaner signal to work with. That is it. That is the whole thing.
This is education, not diagnosis. Persistent pain always deserves appropriate medical screening when red flags are present. Your job here is to run safe, respectful experiments that improve clarity, reduce threat, and help the client find better options.
Go try it. Report back. You've got this.
I love you, take care of those nervous systems out there! See you in a month,
Missy B
References
Tactile acuity and chronic pain systematic review: pubmed.ncbi.nlm.nih.gov/24983492
Tactile discrimination vs. stimulation in chronic limb pain: pubmed.ncbi.nlm.nih.gov/18054437
Tactile discrimination training plus visual context in CRPS / phantom limb pain: pubmed.ncbi.nlm.nih.gov/19501965